Dental Restorations Part 5: Metal-Ceramics or All-Ceramics
An area where looks, quality, and reliability combine is in a metal and ceramic blend called a Porcelain Fused to Metal (PFM) restoration, or a Metal Ceramic Restoration (MCR) — two terms for the same thing.


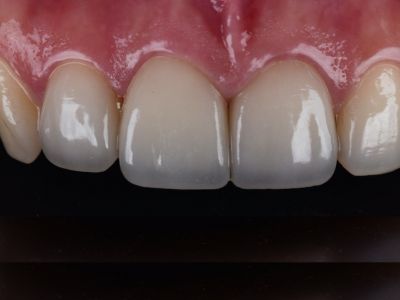
These are possible for crowns and bridges, and have been used in dentistry for more than 60 years. The tongue side of the restoration can be metal, with the visible side being white ceramic. This can be modified by personal preferences, even making the entire crown tooth-colored on the outside and metal on the inside. A common claim is that all-ceramic options make the best tooth-colored crowns or bridges. This is not entirely so. Many don't know that a PFM/MCR crown or bridge can be made to replicate the same high esthetic parameters as well. Crowns from either design can appear identical from the front. The pictures below show different sets of PFM crowns on the left three teeth. The shades are different for different cases, with varying esthetic demands, and abilities. Some choose to cover the front 4-6 teeth to get a completely identical color.

Many are surprised to learn both crown sets above have metal in them. PFMs (MCRs) can be a best of both worlds option. The metal provides strength, while the ceramic provides appearance. These metal-ceramic crowns use a softer type of ceramic that is strengthened by the metal underneath - reducing the risk for this ceramic to wear down opposing teeth. The cement used to adhere this type of crown to a tooth also accomplishes incredible retentive strength, and these crowns are simple to remove if replacement is needed because the metal is discernible from tooth structure underneath. These restorations also have a nice backup function, in that the metal remains if the outer ceramic fractures. That means there is no chance for a total through-fracture, which exists with all ceramic options. As a result, the fracture can often be polished and the restoration continues working.
PFM (MCR) restorations are common, although they are being replaced by all-ceramic alternatives. All-ceramic restorations are the newest version of inlays, onlays, crowns, and bridges that used to be dominated by metal, or PFM/MCR options. These ceramic restorations have been growing rapidly in popularity over the last 15-20 years. This is driven by a number of reasons, including people desiring completely tooth-colored options, newer ceramics having several distinct superior properties, the ability to be produced in greater number and at lower costs due to the use of machines, and increases in ceramic strength that previously were not possible.


Depending on the different types of ceramic, the strength can vary. Ceramics of middle-range strength are common for inlays, onlays, veneers, and some crowns. In some cases, all-ceramic restorations can have a greater risk for fracture. As a result, more tooth structure may need to be removed to increase the ceramic thickness. This leads to a greater risk for the tooth becoming sensitive and potentially needing a root canal. The highest strength ceramics used in dentistry can avoid this, and involve a material known as zirconia. This is similar to what artificial diamonds (cubic zirconia) are made from. Dental zirconia-based restorations are heated at different temperatures, and have different materials — but the strength translates. You can hit some types of these restorations with a hammer and they won’t break. The strength of zirconia lets it perform similar to a metal, while retaining a white tooth color.
It is important to note, just because a crown may be called zirconia, does not mean it is a zirconia with the full properties just mentioned. Zirconia is placed in varying amounts depending on the ceramic. If a ceramic is part zirconia, it could be described as "zirconia". True zirconia ceramic crowns/bridges that can perform with the greatest strength and durability similar to a metal must be made with a certain amount of an ingredient known as yttrium oxide. A problem with dental ceramics since the start of their existence has been their risk for fracturing, and with zirconia, this is very dependent on the percentage of yttrium oxide, or "yttria" in the material.
A zirconia restoration with a 3 mole percent yttria typically yields the strongest zirconia restoration, and is referred to in dentistry as "3Y". Practically speaking, this is the strongest all-ceramic option that exists, and this material has been the breakthrough when combining strength and esthetics. The tradeoff is these restorations can be very opaque, and not look as lifelike, or translucent, as a natural tooth. As a result, more esthetic variations of zirconia exist, raising the mole percent yttria to 4, 5, 6, 7, 8, and even 9Y. While beautiful, the strength goes down as the Y percent goes up. The reason this is relevant is because a crown may be generically referred to as "zirconia", however the specific type and properties of the zirconia one receives need to be specified and chosen to fit expectations.
Regarding adhesion to a tooth, this is the last detail where modern ceramics differ from past options involving metal. Many ceramics have the ability to be traditionally cemented to a tooth similar to MCR/PFM or all-metal option, but the cement may have difficulty holding the ceramic restoration on the tooth. This is not a problem with MCR/PFM or metal options because the metal can be roughened on the inside, and the cement gets GREAT retention. If you roughen a ceramic, however, you induce microscopic cracks that increase the risk of fracturing. So the inside of the ceramic can only be altered so much, if at all. It ends up being pretty sleek and shiny. So classic cements have a harder time holding to the restoration. As a result, an all-ceramic restoration may have a greater risk for coming off a tooth. That being said, as long as the tooth structure is generous in size, and designed by the dentist for maximum retention, the problem may be avoided entirely.
Another solution to ceramic restorations coming off a tooth involves adhesively bonding them to the tooth - basically using a very hard, strong glue capable of adhering to ceramic - which can be an advantage or a disadvantage. In the same way bonded composites can be affected, so too can adhesive agents. Acidic foods (such as tomatoes, oranges, lemons, etc), drinks (coffee, soda, orange juice, etc), and plaque can cause adhesives to be particularly vulnerable. Metabolism of the bonding agent from enzymes in the tooth will also occur over the restoration's lifespan. So it is a consideration to be weighed.
Regarding cracks or fractures, any tooth-colored restoration can fracture. A MCR/PFM restoration can have a greater risk for the ceramic fracturing off the metal substructure, and this is a risk that must be deliberated alongside other benefits of the metal/ceramic hybrid design. Zirconia restorations with their profound strength have a much better ability to resist fracturing. So in short, if there is a risk for a crown coming off a tooth, an MCR/PFM can hold very tightly to the tooth with classic cement. If there is a risk for the crown breaking, a zirconia crown can reduce that risk, while also performing excellent with classic cement.
Ceramic crowns represent the newest generation of dental technology, and offer enormous possibility for treatment. A digital, 3-D manufacturing machine is typically used to make these restorations, rather than a human who physically sculpts the material. As a result, ceramic restorations can be produced efficiently and with constant accuracy. All-ceramic options can have low-cost and expensive versions. It all depends on who makes them and how they do it. In the current world with large businesses involved in dentistry, cost-cutting, and other factors, you have to make sure your dental materials are made with excellent quality control. Low-cost or cheap dental options tend to be made with lesser-grade materials, as well as oversight, and these restorations can be particularly easy for labs in other countries to make and import for an additionally low cost.
With advances in material science, ceramics have become more predictable and offer excellent clinical results. Modern technology now allows them to look great, have long-term performance, and offer new benefits contributing to their overall success. With more materials being employed in dentistry, esthetic and durable treatment is more possible than ever before.